Bilirubin terminology may be challenging for some learners. A helpful tip may be to remember English grammar: VOWELS for B1 (indirect, unconjugated, insoluble) CONSONANTS for B2 (direct, conjugated, water-soluble) While some studies reported direct and indirect terminology is outdated, the truth of the matter is that this terminology is still commonly used in the clinical laboratory today.
Bishop, M. L. (2022). Clinical Chemistry: Principles, Techniques, and Correlations (9th ed.). Jones & Bartlett Learning.
A comprehensive review of relevant topics in the international certification exams for Medical Technologists such as the ASCPi (may also be used for AIMS and CSMLS).
Validity of Subscription:
Your subscription will be VALID UNTIL COVID-19 PANDEMIC ENDS* OR UNTIL YOU TAKE YOUR INTENDED EXAM, WHICHEVER IS SOONER
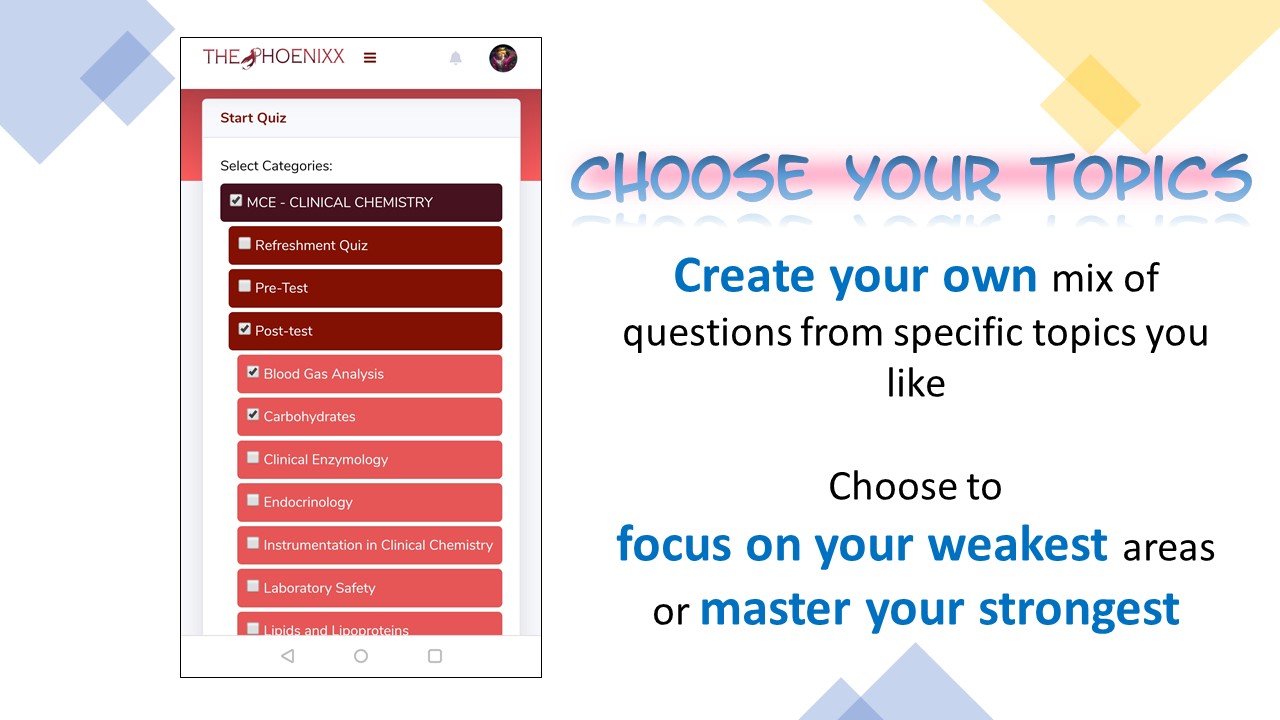
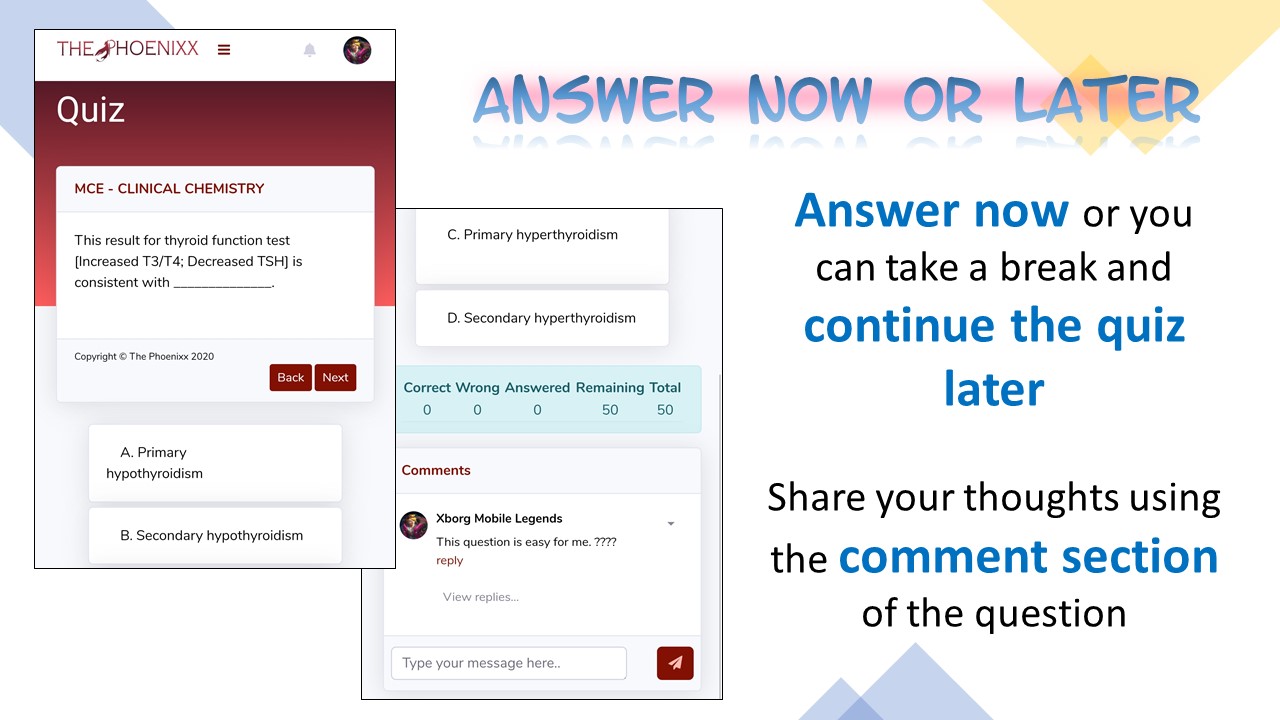
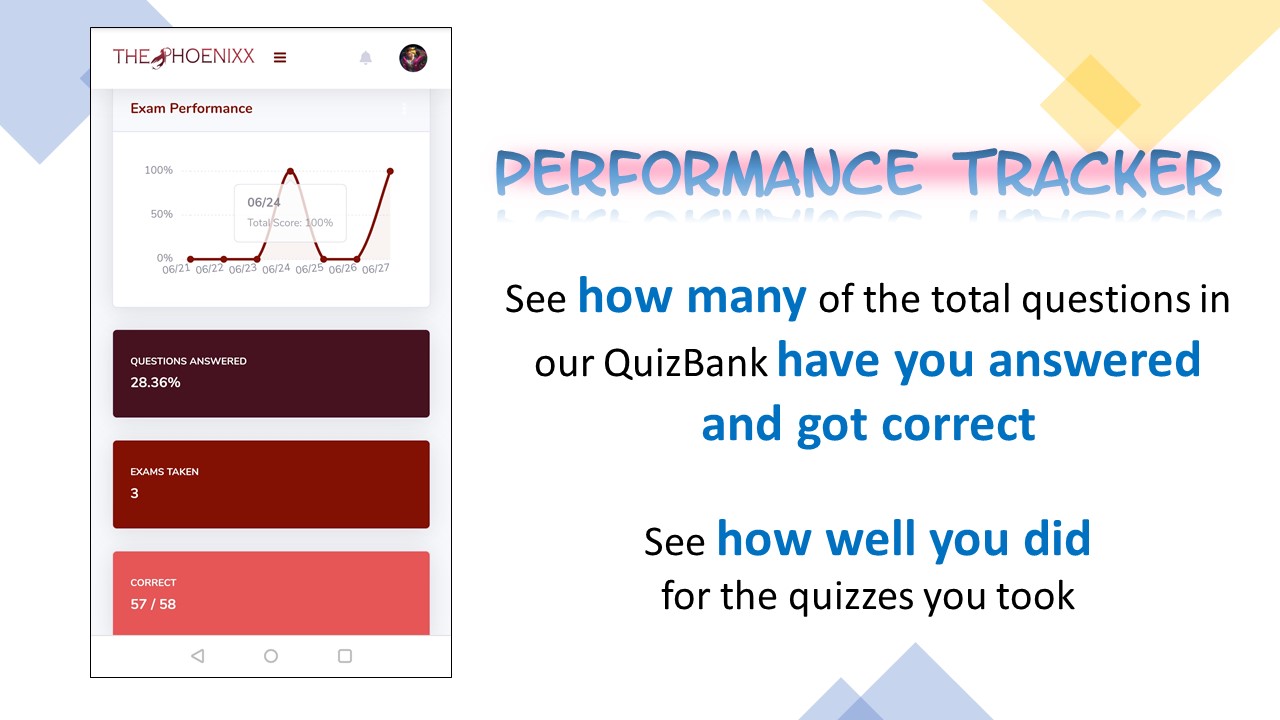
Practice exams/quizzes with feedback, item analysis and progress tracker
More in-app features to help you be more productive
Printable and annotatable soft copy of personalized PCE Notes
Comprehensive exams and practice quizzes
Final Coaching Session with notes
IMPORTANT: APPLICATION ASSISTANCE NOT INCLUDED (We may answer questions you may have but you will have to personally apply for the exam. For more information, please check these links.)
Proof of payment (screenshot of transaction or photo of deposit slip/receipt)
Decent photo to be used for digital ID (preferably graduation pictures)
Slots for enrollment are unlimited. We can always accomodate you and your friends.
1) When you join, YOU AGREE TO THE FOLLOWING TERMS & CONDITIONS. a. No recording in any form (audio, video, screenshot) will be allowed. Programs are in place to monitor your in-app activity and once you’ve violated our agreement, we will be compelled to file charges against you. b. Your personal information will be kept strictly confidential and will not be sold, reused, rented, loaned or otherwise disclosed. c. Only fully paid students will be allowed to join. Please BE HONEST and DO NOT invite students to join without paying individually.
2) To proceed with enrollment, please pay first using the following modes of payment. Fees are NON-REFUNDABLE and NON-TRANSFERABLE.
BANK DEPOSIT BANCO DE ORO (BDO) ACCOUNT NAME: Krizza-Almond S. Aguilar ACCOUNT NUMBER: 00 732 001 4669
SECURITY BANK (SB) ACCOUNT NAME: Krizza-Almond S. Aguilar ACCOUNT NUMBER: 00000 17563681
GCASH (See QR code below) If GCASH to GCASH or GCASH to bank, no extra fee If kiosk (i.e., 7-11, palawan) to gcash, please add the required service fee to the amount to be transferred GCash via PALAWAN: add 2% service fee GCash via 7-11: add 3% service fee
PLEASE DO NOT SEND PAYMENT VIA PALAWAN PERA PADALA. HUWAG MAGPADALA SA PALAWAN EXPRESS PERA PADALA.
3) Register using this PCE form. Please make sure you have the proof of payment ready as well as a decent photo which we will be using for your digital ID.
4) Wait for confirmation via text or email along with the instructions. Sir Axel will assist you. Kindly wait for his message.
5) Review notes (watermarked with your names) are included in the fee and will be sent in digital/soft copy via email/messenger. Please DO NOT SHARE them to anyone WITHOUT PERMISSION.
If you still have any questions or clarifications, please contact me. Thank you very much and looking forward to meeting you online. 😊
Thank you very much and looking forward to meeting you online. 😊
Advertisements
ALSO AVAILABLE! Get 50% discount if you enroll in both MCE and PCE courses.
FIRST, if you are too lazy to read everything here, then my tutorial is not for you. I’m sorry.
SECOND, if you are a fresh graduate/first timer, I suggest that you try in a review center first. But if you insist to join us, you are more than welcome.
THIRD, I do not accept everyone. I only want to do this for those who are fully willing to help themselves too. If you are looking for spoon feeding type of learning then I’m not the one who can help you.
FOURTH, please be aware that this is NOT the usual tutorial set-up nor the usual review center set-up you know…As in everything is NOT the usual.
FIFTH, please bear in mind that I am not forcing you to join. If you find it in your heart that you really want to do your review with us, then we are waiting for you. But if you don’t like any of the above rules, then thank you for your time.
There are a lot to explain (and some are really not explainable by words) but here’s a runthrough of #CheckPoint tutorials.
CheckPoint Tutorials for March 2019 will start on November 2019. Actual dates will be announced when PRC releases the final board exam dates.
We are currently having the tutorials in 2 areas.
CheckPoint Manila version 10.0
CheckPoint Davao version 3.0
We don’t meet everyday.
Our schedule is not fixed since we (the tutors) are also working and so we will be developing a schedule that fits everybody.
Venues
CheckPoint Manila: OUR HOME at SAN MIGUEL (or PALATIW), PASIG CITY
We have a room for tutorials just in front of our home. I am very sorry if I cannot grant your request to do the tutorial anywhere other than this venue.
CheckPoint Davao: No permanent venue as of yet, we usually do tutorials in different coffee shops around Davao. 🙂
I do the teaching but I also get help from my colleagues.
CheckPoint Manila: I do most of the teaching but there’ll be subjects to be handled by Sir Ross Axel Rufino (Unciano Colleges).
CheckPoint Davao: Most subjects will be handled by Sir Jayson Sanchez (Davao Doctors College) while I teach certain subject/s whenever I have a schedule in Davao.
We have a tradition not to move to another topic until everyone in the group understands. And yes, you can tell us everything you want to understand and we will try our best to explain but we don’t guarantee being all-knowing. If we don’t know the answer to your question, then we are willing to study again for you.
If you want an easy life and would just want to rely on recall questions, then you’re in the wrong place.
You will pass because you understood the topics, not because you remember the recalls. But if you believe otherwise, then I can’t help you. That’s not how I roll.
We will also have a lot of practice exams with explanations why this and not that is the answer moments.
There will be unpleasant moments (typhoon, super traffic, dysmenorrhea days) to teach personally so that we’ll just have an online review.
I will require at least 50% downpayment for our expenses.
FEE: Manila – P11,000 & Davao – P12,000 (already inclusive of P1,860 worth of personalized #CheckPoint Notes – all available subjects)
I am not rich, I cannot support our growing #CheckPoint family with just my usual budget so, please pay. Haha. Usually, I use the money for our refreshments (food and coffeeeeee) and enjoyment (like ice skating, karaoke, arcades, haha, no kidding).
I DO NOT ACCEPT QUITTERS.
If you are joining us, make sure that you are not a quitter or if you really are, be prepared to change. To tell you the truth, I’m not willing to do this for someone who will QUIT on me, so, let’s have a contract as early as now.
I do this because I live to teach.
This has been my passion ever since and has been a part of my promise to my God (long story, you’ll know on the way). I choose to teach MedTech students who are willing to sacrifice, change for the better, believe in themselves and fight for their dreams. Even if it is hard, we will not quit.
Description: A course that aims to provide a comprehensive review of topics PER BOARD EXAM SUBJECT based on the Updated PRC Table of Specifications.
Highlights and Inclusions:
REVIEW STYLE OPTIONS:
Scheduled review
If you like interacting with the lecturer, review assistants, and your online study buddies, join our scheduled review.
Live Sessions: 9am to 6pm
See our schedule below
Self-paced review
If you are working, or still an undergraduate, or simply prefer to study by your own, you can do self-paced review.
Hybrid review (combined scheduled and self-paced)
If you wish to do both, you can.Just maintain your communication with us so we can help you in any way we can.
VALIDITY OF ENROLLMENT:
Your enrolled subject/s will be VALID UNTIL COVID-19 PANDEMIC ENDS* OR UNTIL YOU TAKE THE BOARD EXAM, WHICHEVER IS SOONER
*Once the pandemic ends, 1-year validity will follow
Example scenario: If you enroll today (March 2022) but you plan to take the board exam on March 2023, you can join all the batches of the review with no additional cost. (This offer is valid only during the COVID-19 pandemic.)
ENROLLMENT OPTIONS:
Per subject
Choose this option if you just want to enroll in selected subject/s only or if you do not have the budget yet for a full course review.
Full course
Choose this option if you wish to access all subjects right away.
Get a FREE END CELL EDITION (ECE) COURSE – THE ONLINE FINAL COACHING when you enroll in all subjects (whether in a full course or per subject basis)
Practice exams/quizzes with feedback, item analysis, and a progress tracker
More in-app features to help you be more productive
Printable and annotatable soft copy of personalized MCE Notes and other review materials
Every subject (except MolBio*) will have the following academic activities(to be explained in detail during orientation)
MCE Lectures
Pre and Post-lecture Exams
Evaluation Exams with rationalization
Enhancement Exams with rationalization
Mastery Sessions
Drills
Special lectures for selected subjects
*MolBio will only include pre/post-test, lecture, and enhancement exams
GENERAL ACTIVITIES
Co-MEMORY-ate
Mock Board Examination
Brainstorming sessions or virtual group study sessions (Study-With-Me via Discord)
Small group tutorial (by request)
EXTRA-CURRICULAR ACTIVITIES
Worship service/Bible studies
Mental health hygiene
Support group
Chillout sessions
ZOOMba sessions
Gaming sessions
Schedule and Review Fees for AUGUST 2024 MCE:
Dates include INDEPENDENT STUDY TIME (ISTs) or FREE DAY
NO SUNDAY CLASSES
You can register now and access the review materials that are already available. Then, you can join the new batch for March 2024 when it begins in November without paying extra.
UNDERGRADUATES ARE WELCOME TO ENROLL.
ACTIVITY
TARGET DATES
REVIEW FEE
REFRESHMENT WEEK
May 12 to 18, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
MENTAL HEALTH SESSION
May 17, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
GENERAL ORIENTATION
May 18, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
OPENING WORSHIP NIGHT
May 19, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
CC
May 19 to 29, 2024
P3100
BMVP (Bacte, MycoViroPara)
May 30 to June 10, 2024
P3100
CM
June 11 to 18, 2024
P1600
HEMA
June 19 to 28, 2024
P3100
ISBB
June 29 to July 9, 2024
P3100
HTMLE
July 10 to 17, 2024
P1600
MOLECULAR BIOLOGY*
July 18 to 19, 2024
P1600
Drills
July 20, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
MOCK BOARDS
July 22 and 23, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
Co-MEMORY-Ate
August 3, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
GRAND WORSHIP DAY AND SEND-OFF
August 5, 2024
FREE FOR ALL MEMORY CELLS AND END CELLS
TOTAL FEE
All schedules inclusive of lecture days, ISTs, exams, ratio, and mastery sessions except MolBio (only includes lectures, notes, and enhancement exams)
P17,200*
TARGET SCHEDULE OF ACTIVITIES FOR AUGUST 2024 MTLE REVIEW *PRICES WILL INCREASE ON AUGUST 1, 2024. Enroll before August 1, 2024, to avail the current prices.
Watch this for a more detailed explanation of the MCE review course.
STEPS FOR ENROLLMENT
REQUIREMENTS:
Proof of payment (screenshot of transaction or photo of deposit slip/receipt)
Decent photo to be used for digital ID (preferably graduation pictures)
Slots for enrollment are unlimited. We can always accommodate you and your friends.
To get the materials ahead of schedule, please enroll at least 3 days before the subject starts (see schedule here)
If you were not able to enroll on time, you may still register any time and use ThePhoenixxAppto replay the video lectures
1) When you join, YOU AGREE TO THE FOLLOWING TERMS & CONDITIONS. a. No recording in any form (audio, video, screenshot) will be allowed. Programs are in place to monitor your in-app activity and once you’ve violated our agreement, we will be compelled to file charges against you. b. Your personal information will be kept strictly confidential and will not be sold, reused, rented, loaned, or otherwise disclosed. c. Only fully paid students will be allowed to join. Please BE HONEST and DO NOT invite students to join without paying individually.
2) To proceed with enrollment, please pay first using the following modes of payment. Fees are NON-REFUNDABLE and NON-TRANSFERABLE.
You can pay on a full or per subject basis. (SEE THIS FOR FAQs ABOUT PAYMENT) To be able to get the materials on time, please enroll at least 3 days before the start of the subject/s.
If the subject/s you are enrolling in is/are already finished, you can still enroll any time as you wish and you will just be replaying the lectures in the app.
BANK DEPOSIT BANCO DE ORO (BDO) ACCOUNT NAME: Krizza-Almond S. Aguilar ACCOUNT NUMBER: 00 732 001 4669
SECURITY BANK (SB) ACCOUNT NAME: Krizza-Almond S. Aguilar ACCOUNT NUMBER: 00000 17563681
GCASH (See QR code below) If GCASH to GCASH or GCASH to bank, no extra fee If kiosk (i.e., 7-11, palawan) to gcash, please add the required service fee to the amount to be transferred GCash via PALAWAN: add 2% service fee GCash via 7-11: add 3% service fee
PLEASE DO NOT SEND PAYMENT VIA PALAWAN PERA PADALA. HUWAG MAGPADALA SA PALAWAN EXPRESS PERA PADALA.
3) Register using this MCE form. Please make sure you have the proof of payment ready as well as a decent photo which we will be using for your digital ID.
4) Wait for confirmation via text or email along with the instructions. Sir Axel will assist you. Kindly wait for his message.
Enroll in all subjects and automatically get a free online final coaching.
WHO CONDUCTS THE LECTURES?
Dra. Krizza-Almond S. Aguilar-Salido handles all lectures for the 7 subjects but there will be invited special lecturers for a the exam rationalizations and special sessions.
heterotrophic members of the plant family that lack stems and roots
Lack chlorophyll
Larger and with more complex morphology than the bacteria
Chitin in the cell wall
Ergosterol in the cell membrane
Saprophytic nature (derive nutrition from organic materials)
Lack of susceptibility to antibacterial antibiotics
TWO PHASES:
Multicellular MOLD – fluffy, cottony, woolly, or powdery mycelial mass, grows at 25°C
Unicellular YEAST – moist, creamy, opaque or pasty, resembling bacterial colony, grows from 35°C to 37°C
DIMORPHIC FUNGI – capable of two phases Mold at 25°C to 30°C – INFECTIVE TO MAN Yeast at 37°C – TISSUE/IN VIVO/INVASIVE
PARTS:
MYCELIUM – intertwining structure composed of tubular filaments known as HYPHAE
Vegetative portion or thallus – grows in or on a substrate and absorbs water and nutrients
Reproductive or aerial part – contains fruiting bodies that produce reproductive structures (conidia or spores); extends above the agar surface
HYPHAE – microscopic unit of fungi
Septate – contain cross-walls
All fungi except Zygomycetes
Aseptate/Coenocytic – continuous, without cross-walls
ZYGOMYCETES (Rhizopus, Mucor)
Advertisements
FUNGAL REPRODUCTION:
SEXUAL – meiosis (reduction division of two fertile cells) followed by merging of the cells and nuclear fusion occurs
PERFECT FUNGI – fungi that exhibit sexual phase
ASCOSPORES – contained in a saclike ASCUS
CLEISTOTHECIUM – large, round, multicellular structure that surrounds the asci until it ruptures, releasing ascospores
BASIDIOSPORES – contained in a club-shaped BASIDIUM
OOSPORES – fusion of cells from two separate, nonidentical hyphae
ZYGOSPORES – fusion of two identical cells arising from the same hypha
ASEXUAL – involves only mitosis with nuclear and cytoplasmic division
IMPERFECT FUNGI – do not exhibit sexual phase
SPORANGIOSPORES – asexual spores contained in sporangia (sacs) and produced terminally on sporangiophores or aseptate hyphae
UNIQUE TO THE ZYGOMYCETES
CONIDIA – asexual spores produced either singly or multiply in long chains or clusters by specialized vegetative hyphae (conidiophores)
MACROCONIDIA – large, usually septate
Club, oval, or spindle shaped
Thick or thin walled
Spiny (echinulate) or smooth surface
MICROCONIDIA – small, unicellular
Round, elliptical, or pyriform (pear) shape
BLASTOCONIDIA or BLASTOSPORES
Develop as daughter cell buds off the mother cell and is pinched off
Blastoconidia of yeasts (including Candida) may elongate to form pseudohyphae
CHLAMYDOCONIDIA or CHLAMYDOSPORES
Thick-walled, resistant, resting spores produced by “rounding up” and enlargement of the terminal hyphal cells
Germinate into a new organism when favorable environmental conditions exist
Terminal – form at the hyphal tip
Sessile – form on the hyphal sides
Intercalary – form within the hyphal strand
ARTHROCONIDIA or ARTHROSPORES
Simple fragmentation of the mycelium at the septum into rectangular-, cylinder-, or cask-shaped spores
Thick walled spores which may be adjacent or alternate (empty spaces or disjunctor cells in between each arthrospores) in arrangement
Useful identification characteristic of Coccidioides immitis and Geotrichum candidum
CLASSIFICATION
Botanical Taxonomy
Zygomycota –Mucor, Absidia, Rhizopus
Ascomycota
Basidomycota
Deuteromycota – most medically important fungi
With septate hyphae
Asexual reproduction
Type of Mycoses
Superficial and cutaneous mycoses
Subcutaneous mycoses
Systemic mycoses
Opportunistic mycoses
Advertisements
IDENTIFICATION METHODS
MICROSCOPIC
SALINE MOUNT – quick and simple method to observe fungal elements (budding yeast, hyphae, pseudohyphae)
Major disadvantage: Lack of contrast
10% KOH PREPARATION – rapid and simple method to examine hyphae, budding yeast and spherules
KOH dissolves keratin in skin, hair, or nail
Chitin is resistant to effects of KOH
Hair can be examined to determine type of infection
ENDOTHRIX – fungal invasion within the hair shaft
ECTOTHRIX – infection outside the hair shaft
Disadvantage: Lack of contrast
CELLUFLUOR – chemofluorescent brightening agent
Can be added to the KOH solution
Binds to the chitin in fungal cell wall
Provides excellent contrast when examined with a fluorescent microscope
Fungi fluoresce intense apple green
INDIA INK/NIGROSIN – used to identify hyaline capsule of the yeast Cryptococcus neoformans
Capsules do not stain with India ink and appear as clear halos against a dark background
May be difficult to interpret; WBCs and artifacts can be mistaken for yeast or capsules
Cryptococcus may be capsule negative in immunodeficiency
Replaced by direct antigen testing for the cryptococcal capsular protein
LACTOPHENOL COTTON BLUE (LPCB) (AMAN) – imparts blue color to the fungal cell wall
Slides can be permanently sealed for later study with either Permount or clear nail polish
Can also be used in the tease preparation (wet mount) and slide cultures
HUCKER MODIFICATION OF GRAM STAIN – recommended for mycology
Fungi generally stain gram positive
Oval or budding yeast, hyphae, arthrospores generally stain well
C. neoformans may appear pale lavender with blue inclusions (capsule prevents adequate staining)
Fungi are 2 to 3x the size of gram-positive cocci
Hyphae are 2 to 3x wider than gram-positive bacilli
GIEMSA or WRIGHT’S STAIN – used for the detection of intracellular Histoplasma capsulatum in blood smears, lymph nodes, lung, liver, or bone marrow
H. capsulatum appears as small, oval yeast cell staining light to dark blue
C. neoformans also stain well
METHENAMINE SLIVER NITRATE STAIN – useful for screening of clinical specimens
Provides good contrast and staining for fungal elements
Fungi appear outlined in black, with an inner dark rose to black color against a pale green background
Viable and nonviable fungi are stained using this method
GOMORI METHENAMINE SILVER (GMS) NITRATE MODIFICATION – used in histology to detect fungi in specimens
PERIODIC ACID SCHIFF (PAS) – stains hyphae of molds and yeast
Periodic acid oxidizes the hydroxyl in the carbohydrates of the cell walls to form aldehydes which react with basic fuchsin dye to form a pink-purple complex
Counterstain of fast green can be used to provide contrast
Useful in staining tissue in histology
CULTURE
Must include a source of nitrogen (nitrite, nitrate, amino acids, or urea) and a carbon source (usually glucose)
SABOURAUD DEXTROSE AGAR (SDA) Main general isolation medium Primary recovery of saprobic and pathogenic fungi Primary agar for initial culture Contains peptone and glucose Inhibitor for bacteria: ACIDIC pH (5.6)
SDA WITH CYCLOHEXIMIDE AND CHLORAMPHENICOL (SDA-CC) Recovery of pathogenic fungi Bacteria and saprophytic fungi inhibited Available commercially as Mycosel or Mycobiotic medium
MYCOSEL OR MYCOBIOTIC AGAR Isolation of dermatophytes from hair, skin, and nail specimens Contains the inhibitory agents, cycloheximide and chloramphenicol Similar to DTM
DERMATOPHYTE TEST MEDIUM (DTM) Can be substituted for SDA-CC for the recovery of dermatophytes from specimens contaminated with fungi or bacteria Isolation of dermatophytes from hair, skin, and nail specimens Dermatophytes produce alkaline metabolites, which raise the pH and change the color of the indicator from yellow to red Indicator: PHENOL RED Antibiotics inhibit saprophytic fungi and bacteria
BRAIN-HEART INFUSION (BHI) AGAR Isolation of saprophytic and pathogenic fungi from sterile sites Bacteria also grown in BHI Can be supplemented with blood
BHI AGARWITH ANTIBIOTICS, CYCLOHEXIMIDE AND CHLORAMPHENICOL Isolation of pathogenic fungi exclusive of dermatophytes; useful for specimens that may be contaminated with bacteria or saprophytic fungi
BHI BIPHASIC BLOOD CULTURE BOTTLES Recovery of fungi from blood or bone marrow
DIFFERENTIAL MEDIA
BIRDSEED (NIGER SEED) AGAR/ STAIB’S MEDIUM Isolation of Cryptococcus neoformans: brown to black colonies in 4 to 7 days C. neoformans produces phenol oxidase which breaks down the medium resulting in the production of melanin Similar to caffeic acid agar
CORNMEAL AGAR WITH TWEEN 80 Stimulation of conidiation and chlamydospore production in Candida species; useful for species differentiation of Candida Cornmeal agar + 1% glucose: differentiates T. rubrum from T. mentagrophytes based on PIGMENTATION
COTTONSEED AGAR Conversion of mold phase of Blastomyces dermatitidis to its yeast phase
NITRATE REDUCTION MEDIUM Confirmation of nitrate reduction in C. neoformans
POTATO DEXTROSE AGAR Stimulation of conidia production in fungi Useful in slide culture Also demonstrates pigment production of Trichophytonrubrum
RICE MEDIUM Identification of Microsporum audouinii
TRICHOPHYTON AGARS Nutritional requirement tests for the differentiation of Trichophyton #1: casein agar base (vitamin free) #2: casein agar base and inositol #3: casein agar base, inositol, and thiamine #4: casein agar base and thiamine #5: casein agar base and nicotinic acid #6: ammonium nitrate agar base #7: ammonium nitrate agar base and histidine
UREA AGAR Detection of urease production by C. neoformans and differentiation of Trichophyton mentagrophytes from T. rubrum
YEAST ASSIMILATION MEDIA (CARBON OR NITROGEN) Detection of carbohydrate assimilation through utilization of carbon (or nitrogen) by yeast in the presence of oxygen
YEAST FERMENTATION BROTH Identification of yeasts by fermentation reactions with various carbohydrates
Glucose (correlated with ketones) Double sequential enzyme reaction
ENZYMES: Glucose oxidase Peroxidase
30 s
M – glucose oxidase, peroxidase, potassium iodide C – glucose oxidase, peroxidase, tetramethylbenzidine
CHROMOGENS: O-toluidine (pink to purple) Potassium iodide (blue to brown) Aminopropryl-carbazol (yellow to orange-brown) Tetramethylbenzidine (yellow to green)
Contamination by oxidizing agents and detergents
High levels of ascorbic acid, ketones, specific gravity Low temperature Improperly preserved specimens
Ketones (correlated with glucose)
Sodium nitroprusside reaction
40 s
M – sodium nitroprusside (acetoacetic acid)
C – sodium nitroprusside + glycine (acetoacetic acid & acetone)
Phthalein dyes, highly pigmented red urine, levodopa Medications containing free sulfhydryl groups (MESNA)
Improperly preserved specimens
Specific Gravity
pKa change of polyelectrolyte
pKa = dissociation constant
45 s
M – poly (methy lvinyl ether/maleic anhydride) bromthymol blue
C – ethyleneglycol-Bis (aminoethylether) bromthymol blue
High concentrations of proteins because of protein anions
Highly alkaline urines (>6.5) Add 0.005 to S.G. readings
pH (correlated with Nitrite, LE, microscopic)
Double-indicator system
60 s
Methyl red Bromthymol blue
None
Runover from the adjacent CHON pad may lower pH
Protein (correlated with blood, nitrite, LE, microscopic)
Protein error of indicators
60 s
M – tetrabromphenol blue
C – tetrachloropenol tetrabromosulfonphthalein
ACID BUFFER: Citrate
Highly buffered alkaline urine High specific gravity pigmented specimens, phenazopyridine quaternary ammonium compounds (detergents) antiseptics, chlorhexidine loss of buffer from prolonged exposure of reagent strip to the specimen
Proteins other than albumin
Blood (correlated with protein and microscopic)
Pseudo-peroxidase activity of hemoglobin
60 s
M – diisopropylbenzenedehydroperoxide tetramethylbenzidine
C – dimethyldihyroperoxide- tetramethylbenzidine
spotted blue for intact RBCsuniform blue for Hb and myoglobin
C – old specimens, preservation in formalin, high concentration of nitrite
Nitrite (correlated with protein, LE and microscopic)
Greiss reaction
60 s
M – p-arsanilic acid Tetrahydrobenzo(h)-quinolin-3-ol
C – Sulfanilamide, hydroxytetrahydro benzoquinoline
Improperly preserved specimens
Highly pigmented urine
Nonreductase-containing bacteria insufficient contact between bacteria and urinary nitrate (should be 4 hours) lack of urinary nitrate, large quantities of bacteria converting nitrite to nitrogen, presence of antibiotics, high concentration of ascorbic acid high specific gravity
Leukocytes (correlated with protein, nitrite and microscopic)
Leukocyte esterase
120 s
M – derivatized pyerole amino acid ester, diazonium salt
Principles Used in Automated Urinalysis and Microscopy
Automated Urinalysis Systems
Automated Body Fluid Analysis Systems
Principles Used in Automated Urinalysis and Microscopy
REFLECTANCE PHOTOMETRY
Used by automated reagent strip readers
Measure the light reflected from the reagent strip color pads and compare the amount of reflected light with a known standard
PRINCIPLE: light reflected from the colored reagent pads DECREASES in DIRECT PROPORTION to the INTENSITY OF THE COLOR produced by the reaction with the specific substance in the urine sample
the darker the color, the less light reflected
the lighter the color, the more light reflected
The concentration of a specific substance and concentration units are displayed on the reader’s display
Conductivity is based upon the impedance (the amount of resistance that occurs when a sediment passes through an electrical field) of sediments and counts the numbers of pulses (sediments).
The size of the pulse indicates the size of the sediment.
Light scattering characteristics of the sediments are determined by their movement through the laser light beam.
Identification depends on how the light is scattered by the sediment.
HARMONIC OSCILLATION
Assesses SPECIFIC GRAVITY
Method based upon densitometry in which a sound wave of a specific frequency changes in proportion to the density of the urine sample
Change in wave frequency is measured by a microprocessor and translates the reading to specific gravity
HYDRODYNAMIC FOCUSING
Identifies specific sediments
involves the movement of single urine sediments past the optics of a microscope to allow sediments to flow in several planes plane past the microscope objective
A flow cell also measures sediment conductivity, size, and light scattering traits
Questionable findings are viewed on a monitor for operator identification and confirmation
Automated Urinalysis Systems
INDIVIDUAL STRIP READERS
SEMIAUTOMATED ANALYZERS
dependent on an operator for specimen mixing, test strip, dipping, and inputting of physical and microscopic results
FULLY AUTOMATED CHEMISTRY ANALYZERS
add urine to the reagent strip
AUTOMATED URINE CELL ANALYZERS
mix, aspirate, dilute, and stain urine to classify urine sediment particles
COMPLETELY AUTOMATED SYSTEMS
perform a complete urinalysis that includes the physical, chemical, and microscopic parts of a routine urinalysis
WAIVED URINE CHEMISTRY INSTRUMENTS
Roche Diagnostics Criterion II Siemens Medical Solutions Diagnostics Clinitek®50 Siemens Medical Solutions Diagnostics Clinitek®101 Siemens Medical Solutions Diagnostics Clinitek®Status
Iris Diagnostics Division iQ®200 Automated Urinalysis System iRICELL2000 (iChem® VelocityTM plus iQ®200ELITETM) iRICELL3000 (iChem® VelocityTM plus iQ®200SPRINTTM) Siemens Medical Solutions Diagnostics ADVIA Urinalysis WorkCell System (Clinitek® Atlas plus the Sysmex UF-100)
Advertisements
DESCRIPTION OF SOME SELECTED INSTRUMENTS
CLINITEK 50 & CLINITEK STATUS
well suited for small volume laboratories and physician’s offices
Memory storage for test results -100 for Clinitek 50 and 200 for Clinitek Status
automated reading of microalbumin-to-creatinine and protein-to-creatinine ratios and human chorionic gonadotropin (hCG)
CLINITEK 200
For medium-volume to large-volume urinalysis laboratories and features a high specimen output of one strip every 10 seconds.
Multistix reagent test strips are used, and the instrument has the ability to report semiquantitative (mg/dL) results or plus (+) and SI units.
The reflectometer is calibrated daily and maintenance is required each day for all areas in contact with urine test strips
SYSMEX UF-SERIES
Fully automated sample analysis with automatic classification of all 10 formed element groups with SCATTERGRAMS and HISTOGRAMS for reference
Laser-based FLOW CYTOMETRY along with impedance detection, forward light scatter, and fluorescence
Sample is stained with 2 dyes
PHENATHRIDINE – orange dye, stains DNA
CARBOCYANINE – green dye, stains nuclear membranes, mitochondria, and negatively charged cell membranes
SYSMEX UF-SERIES
Stained sample is passed through the flow cell, where it is HYDRODYNAMICALLY FOCUSED and presented to a laser light beam that produces fluorescence and light scatter
Particles are identified by measuring the change in impedance of the sediment elements, as well as the height and width of the fluorescent and light scatter signals, which are presented in scattergrams and histograms
iQ 200 Automated Urine Microscopy Analyzer (IRIS)
Automatically analyses and classifies urine particles into 12 categories
Uses AUTO PARTICLE RECOGNITION (APR) software that classifies urine particles in the photographs based on size, shape, texture, and contrast
Automated Body Fluid Analysis Systems
cells are first mixed with reagent fixative and then counted
differentials countingenumerates numbers of neutrophils, lymphocytes, monocytes, and eosinophils
automated cell counters use larger numbers of cells, enhancing precision and accuracy
Siemens Medical Solutions Diagnostics ADVIA120 and 2120
CSF
Sysmex XE-5000 Automated Hematology System
CSF Serous body fluids Synovial fluid
Medical Electronic Systems
Semen
ADVIA120 Hematology System
First automated instrument with an FDA-approved automated CSF assay
Uses flow cytometry, light scatter, and absorbance to count the RBCs, WBCs, and performs a WBC differential that includes percentages and absolute numbers of mononuclear cells and PMNs on samples with >20WBCs/µL
AUTOMATION OF SEMEN ANALYSIS
SQA-V automates sperm counts and motility
has a two-channel measurement system that interacts with a specially designed testing capillary that contains the semen sample
one channel “measures” light absorption and refraction in sperm cells and translates this into concentration
one channel “counts” light interruptions (signals) caused by sperm cells moving across the field of light
In approximately 1 minute, thousands of signals are “read” resulting in exceptional accuracy and precision.
Automating the motility analysis eliminates reader subjectivity and variance among technologists.
AUTOMATION OF URINE PREGNANCY
Quantitative human chorionic gonadotropin (HCG) is one such test that is interpreted by the VEDALAB Easy Reader.
Immunochromatographic rapid test cards are read by the meter using a high-resolution CCD camera.
Integrated software analyzes the images and records the results.
Compounds containing C, H and O with general formula Cx(H2O)y
Contain C=O and –OH functional groups
Derivatives can be formed by addition of other chemical groups such as phosphates, sulfates and amines
Commonly called “SUGARS” and use the suffix –ose
CLASSIFICATION
Based on four different properties
SIZE OF THE BASE CARBON CHAIN
TRIOSES: with three (3) carbons
TETROSES: with four (4) carbons
PENTOSES: with five (5) carbons
HEXOSES: with six (6) carbons
LOCATION OF THE CO FUNCTION GROUP
ALDOSE: has a terminal carbonyl group (O=CH–) called an aldehyde group
KETOSE: has carbonyl group (O=CH–) in the middle linked to two other carbon atoms called a ketone group
STEREOCHEMISTRY OF THE COMPOUND
STEREOISOMERS: have the same order and types of bonds but different spatial arrangements and different properties
ENANTIOMERS: images that cannot be overlapped and are non-superimposable
L-isomer: if the configuration of the highest-numbered asymmetric carbon is on the LEFT or if hydroxyl group farthest from the carbonyl carbon is on the LEFT
D-isomer: if the configuration of the highest-numbered asymmetric carbon is on the RIGHT or if hydroxyl group farthest from the carbonyl carbon is on the RIGHT
NUMBER OF SUGAR UNITS
MONOSACCHARIDES
Simple sugars that cannot be hydrolyzed to simpler form
Examples: glucose, fructose, galactose
DISACCHARIDES
Formed by two monosaccharides joined by glycosidic linkage
Hydrolyzed by disaccharide enzymes (i.e., lactase) produced by the microvilli of the intestine
Examples:
Maltose = 2 β-D-glucose in 1→4 linkage
Lactose = glucose + galactose
Sucrose = glucose + fructose
OLIGOSACCHARIDES
Chaining of 2 to 10 sugar units
POLYSACCHARIDES
Linkage of many monosaccharide units
Yield more than 10 monosaccharides upon hydrolysis
Examples: starch, glycogen
MODELS USED TO REPRESENT CARBOHYDRATES
FISCHER: linear formula where the aldehyde or ketone is at the top of the drawing and can be depicted in the D- or L- form
HAWORTH: cyclic form that is more representative of the actual structure and is formed when the carbonyl group reacts with an alcohol group on the same sugar to form a ring and can be depicted in the α or β form
The only CHO that can be directly used for energy or stored as glycogen
FORMS: ~35% alpha & 65% beta
MAJOR METABOLIC PATHWAYS
EMBDEN-MEYERHOFF PATHWAY or GLYCOLYSIS
Substrate: D-glucose
End-products: 2 moles of PYRUVIC ACID, 2 moles NADH and 2 moles of ATP
Can occur aerobically or anaerobically
If aerobic, pyruvate is formed
If anaerobic, lactate is formed
Other substrates can enter this pathway at various points
Glycerol (from TAG) enters at 3-phosphoglycerate
Fatty acids, ketones and some amino acids are converted to acetyl-CoA
Other amino acids enter as pyruvates or as deaminated α-ketoacids and α-oxoacids
HEXOSE MONOPHOSPHATE SHUNT OR AEROBIC/OXIDATIVE PATHWAY
G6P is converted to 6-phosphogluconic acid which permits the formation of NADPH (important to red cells because they lack mitochondria thus incapable of TCA cycle)
End-products: pentose phosphate, CO2 and NADPH
GLYCOGENESIS
Stores glucose as glycogen
Converts G6P to G1P
G1P → uridine diphosphoglucose→ glycogen by glycogen synthase
GLYCOGENOLYSIS – conversion of glycogen to G6P
PATHWAYS IN GLUCOSE METABOLISM
Glycolysis
Metabolism of glucose molecule to pyruvate or lactate for production of energy
Gluconeogenesis
Formation of G6P from noncarbohydrate sources
Glycogenolysis
Breakdown of glycogen to glucose for use as energy
Glycogenesis
Conversion of glucose to glycogen for storage
Lipolysis
Decomposition of fats
Lipogenesis
Conversion of carbohydrates to fatty acids
MAJOR HORMONES CONTROLLING BLOOD GLUCOSE
PANCREATIC HORMONES
INSULIN – primary hormone for DECREASING blood glucose levels
Responsible for the entry of glucose into the cells by enhancing membrane permeability to cells in the liver, muscle and adipose tissues
synthesized by β-cells of the pancreas
released when glucose levels are high/increased
not released when glucose levels are low/decreased
EFFECTS:
increases glycogenesis, lipogenesis, and glycolysis
inhibits glycogenolysis
INSULIN IS THE ONLY HORMONE THAT DECREASES GLUCOSE LEVELS and can be referred to as a hypoglycemic agent
GLUCAGON – primary hormone for INCREASING blood glucose levels
released in response to stress and fasting states
synthesized by α-cells of the pancreas
released when glucose levels are low/decreased
not released when glucose levels are high/increased
EFFECTS:
increase glycogenolysis and gluconeogenesis
can be referred to as a hyperglycemic agent
SOMATOSTATIN
produced by δ cells of the pancreas
EFFECTS: inhibition of insulin, glucagon, growth hormone, and other endocrine hormones.
ADRENAL HORMONES
CORTISOL
produced by the adrenal cortex on stimulation by ACTH
EFFECTS: decreases intestinal entry into the cell and increases gluconeogenesis, liver glycogen and lipolysis
EPINEPHRINE
produced by the adrenal medulla
EFFECTS: inhibits insulin secretion, increase glycogenolysis and lipolysis
Released during times of stress
ANTERIOR PITUITARY HORMONES
GROWTH HORMONE
EFFECTS: decreases the entry of glucose into the cells
ACTH
EFFECTS: stimulates the adrenal cortex to release cortisol, increases glycogenolysis and gluconeogenesis
THYROID HORMONES
T3 & T4
EFFECTS: increases glycogenolysis, gluconeogenesis and intestinal absorption of glucose
glycogenolysis, gluconeogenesis & intestinal absorption of glucose
Somatostatin
δ cells of pancreas
↑
inhibits insulin, glucagon, GH
Advertisements
Hyperglycemia
Increase in plasma glucose levels caused by imbalance of hormones
DIABETES MELLITUS
Group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action or both
Categories of Diabetes (According to the ADA/WHO guidelines)
Type 1 Diabetes
Type 2 Diabetes
Other specific types of diabetes
Gestational Diabetes Mellitus (GDM)
PRIMARY DIABETES MELLITUS
Points of Difference
TYPE 1
TYPE 2
Former names
Insulin Dependent Diabetes Mellitus (IDDM)
Juvenile Onset DM
Brittle DM
Ketosis-prone DM
Non-Insulin Dependent Diabetes (NIDDM)
Maturity Onset DM
Stable DM
Ketosis-resistant DM
Receptor Deficient DM
Onset
Before 20 y/o
Over 40 y/o
Measurable circulating insulin
NONE
Low
Insulin receptor
Normal
↓ or ineffective
Beta cell mass
Markedly ↓
Moderately ↓
C-peptide levels
Undetectable
Detectable
Incidence
10-15%
85% (common)
Ketoacidosis*
Common
Rare
Physique/Stature**
Normal or thin
Often overweight
Pathogenesis
-β-cell destruction
-Absolute insulin deficiency
-Autoantibodies
-Insulin resistance with insulin secretory defect
-Relative insulin deficiency
Treatment
Parenteral insulin administraion
Oral hypoglycemic agent
SECONDARY DIABETES MELLITUS – associated with secondary conditions
Genetic defects of β-cell function
Pancreatic disease
Endocrine disease
Cushing syndrome – excessive cortisol
Pheochromocytoma – epinephrine excess
Acromegaly – growth hormone excess
Drug or chemical induced
Insulin receptor abnormalities
Other genetic syndromes
Maturity onset diabetes of youth (MODY) – rare; autosomal dominant
GESTATIONAL DIABETES MELLITUS (GDM)
any degree of glucose intolerance with onset or first recognition during pregnancy
due to metabolic or hormonal changes
Infants born to mothers with this kind of diabetes are at increased risk to respiratory distress syndrome, hypocalcemia & hyperbilirubinemia
Laboratory Findings in Hyperglycemia
INCREASED glucose (plasma & urine), urine specific gravity, serum and urine osmolality
Ketonemia and ketonuria
DECREASED blood and urine pH (acidosis)
Electrolyte imbalance (↓Na+, Cl– and ↑K+)
DIAGNOSTIC CRITERIA FOR DIABETES MELLITUS
RPG ≥200 mg/dl (11.1 mmol/L) + symptoms of diabetes
Fasting PG ≥126 mg/dL (7.0 mmol/L)
2-h PG ≥200 mg/dl (11.1 mmol/L) during OGTT
CATEGORIES OF FASTING PLASMA GLUCOSE
Normal fasting glucose FPG <110 mg/dL
IMPAIRED fasting glucose FPG ≥110 mg/dl but <126 mg/dl
Provisional diabetes dx FPG ≥126 mg/dl
CATEGORIES OF ORAL GLUCOSE TOLERANCE
Normal glucose tolerance 2h PG <140 mg/dL
Impaired gluc. tolerance 2h PG ≥140 mg/dl but <200 mg/dl
Provisional diabetes dx 2h PG ≥200 mg/dl
Screening test for GDM
Only high-risk patients should be screened for GDM
Age older than 25 years
Overweight
Strong family history of diabetes
History of abnormal glucose metabolism
History of a poor obstetric outcome
Presence of glycosuria
Diagnosis of PCOS
Member of an ethnic/racial group with a high prevalence of diabetes (e.g. Hispanic American, Native American, Asian American, African American, Pacific Islander)
METHODS:
ONE-STEP APPROACH – immediate performance of a 3h OGTT without prior screening
TWO-STEP APPROACH – initial measurement of plasma glucose at 1-hour postload (50g)
IF value ≥140 mg/dL (7.8 mmol/L) then do 3-hour OGTT using 100g glucose
GDM is diagnosed when any two of the following values are met or exceeded:
Fasting: >95 mg/dl
1 hour: ≥180 mg/dl
2 hours: ≥155 mg/dl
3 hours: ≥140 mg/dl
Hypoglycemia
Decrease in plasma glucose levels
65-70 mg/dl (3.6-3.9 mmol/L) – plasma glucose concentration at which glucagon and other glycemic factors are released
50-55 mg/dl (2.8-3.0 mmol/L) – symptoms of hypoglycemia appear
Warning S/S are all related to CNS
Types of Hypoglycemia (Old)
Post-absorptive (Fasting) – MORE SERIOUS
Islet cell insulinoma
Insulin-producing tumors
Ethanol induced
Propanolol & salicylate
Post-prandial (Reactive) – MILD FORM
there is spontaneous recovery of glucose level as a result of insulin level returning to normal
Excessive release of insulin
Gastro-intestinal surgery
CAUSES OF HYPOGLYCEMIA
Patient Appears Healthy
No coexisting disease
Drugs
Insulinoma
Islet hyperplasia or NESIDIOBLASTOSIS
Factitial hypoglycemia from insulin or sulfonylurea
Severe exercise
Ketotic hypoglycemia
Compensated coexistent disease
Drugs
Patient Appears ILL
Drugs
Predisposing illness
Hospitalized patient
Diagnostic criteria for INSULINOMA
Change in glucose level of ≥25 mg/dl coincident with an insulin level of ≥6 μU/ml
C-peptide levels of ≥0.2 nmol/L
Proinsulin levels of ≥5 pmol/L
β-hydroxybutyric acid of ≤2.7 mmol/L
Diagnostic tests for HYPOGLYCEMIA
72 hour fast which requires the analysis of glucose, insulin, C-peptide and proinsulin at 6-hour intervals
POSITIVE RESULT: <45 mg/dl; hypoglycemic symptoms appear after 72 hours had elapsed
Advertisements
Genetic Defects in Carbohydrate Metabolism
Glycogen Storage Diseases – deficiency of a specific enzyme that causes alteration of glycogen metabolism
Types
Enzyme Deficient
Clinical Features
von Gierke’s dse
Type I
Glucose-6-phosphatase
Severe fasting hypoglycemia
Lactic acidosis
Pompe’s dse
Type II
α-1,4-glucosidase
Accumulation of ↑ amount of glycogen on all organs
Presence of abnormally LARGE LYSOSOMES
Forbe’s dse
Type III
Debrancher enzyme
Hypoglycemia, hepatomegaly, seizures and mental retardation
Andersen’s dse
Type IV
Brancher enzyme
Progressive liver enlargement or cirrhosis and muscular weakness by age 2
Absence of storage glycogen
Unbranched AMYLOPECTIN
Other enzyme defects/deficiencies that cause hypoglycemia: glycogen synthase, fructose-1-6,biphosphatase, phosphoenolpyruvate carboxykinase and pyruvate carboxylase.
Galactosemia – a cause of failure to thrive syndrome in infants; congenital deficiency of one of three enzymes involved in galactose metabolism, resulting in increased plasma galactose levels
Galactose-1-phosphate uridyl transferase – MOST COMMON enzyme deficiency
Fructose-1-phosphate aldolase deficiency
Laboratory Analysis of Glucose
SPECIMEN COLLECTION AND HANDLING
Glucose concentration in whole blood is approximately 15% lower than in plasma or serum.
Glucose levels decrease approximately 10 mg/dL (7%) per hour in whole blood.
Serum or plasma must be separated within 1 hour (Bishop) to prevent substantial loss of glucose by the cellular fraction, particularly if WBC count is elevated. (within 30 minutes – Henry)
Glucose is metabolized at a rate of 7 mg/dl/h at room temperature; and 2 mg/dl/h at 4°C
Refrigerated serum or plasma is stable up to 48 hours.
Sodium fluoride (2 mg/mL) prevents glycolysis (gray top tube) for up to 48 hours.
Glycolysis decrease serum glucose by approximately 5-7% per hour (5-10 mg/dl) in normal, uncentrifuged coagulated blood at room temperature.
Fasting blood glucose should be obtained after an approximately 10-hour fast (not >16 hours)
Fasting plasma glucose values have a diurnal variation with the mean FBG higher in the morning than in the afternoon.
Fasting reference range for serum or plasma is 70-110 mg/dL
In the fasting state, arterial (capillary) values are 5 mg/dL higher than the venous concentration.
Urine glucose analysis (in 24h urine glucose) may be stabilized by addition of a preservative; should be stored at 4°C during collection because 40% of glucose is lost after 24 hours at room temperature.
CSF glucose analysis (if will be delayed) must be centrifuged and stored at 4°C-20°C
In normal CSF, values are two-thirds (approximately 60-70%) of plasma level.
RENAL THRESHOLD for glucose: 180 mg/dl
TYPES OF SPECIMEN FOR GLUCOSE ANALYSIS
Fasting Blood Sugar – blood collected after 8-10 hours of fasting (NV: 74-106 mg/dl)
Random Blood Sugar – test for INSULIN SHOCK (NV: <200 mg/dl)
2 hour Postprandial Blood Sugar
Standard load of glucose: 75 grams
Glucose measurement taken 2 hours later
(NV : <120 mg/dl)
Glucose Tolerance Test – multiple blood and urine glucose test
Oral GTT
Janney-Isaacson (Single Dose)
Exton Rose (Divided Oral dose or Double Dose)
Not recommended for routine use
Fasting and 2h sample are measured except for pregnant patients
Adult load is 75g; children: 1.75 g/kg to 75g
Factors that affect tolerance
Medications (salicylates, diuretics, anticonvulsants, oral contraceptives and corticosteroids)
GI surgery
Vomiting
Endocrine dysfunction
Requirements:
Patient should be ambulatory
Patient must be in unrestricted diet of 150 grams CHO/day for 3 consecutive days prior to the test
Patient must be free from undue stress or severe illness
Alcohol intake and smoking are not allowed prior to the test
Patient should be fasting at least 10 hours and not more than 16 hours
Test should be performed in the morning because of hormonal diurnal effect on glucose
IVGTT – blood sample is collected every 10 minutes for 1 hour
5g glucose/kg body weight (given within 3 minutes) administered intravenously
fasting is also required
NV: 1.4 – 2.0 %
Indications of IVGTT
Patients who are unable to tolerate large CHO load
Patients with altered gastric physiology or GI d/o
Patients with malabsorption syndrome
Self-Monitoring of Blood Glucose (SMBG)
Type 1 DM – should monitor blood glucose 3-4 times per day
Type 2 DM – optimal frequency is unknown
Glycosylated hemoglobin/Glycated hemoglobin/HbA1C
hemoglobin compound formed when glucose reacts with amino group of hemoglobin
test for long term diabetic control
reflects the average blood glucose level for the previous 2-3 months
for every 1% change in HbA1c value there is 35 mg/dl (2 mmol/L) change in the mean
in presence of hemoglobinopathies, there will be less time for glucose to
binding of glucose to HbA1 is irreversible
preferred anticoagulant is EDTA
NV: 4.5-8.5%
Methods of HBA1c Measurement
Methods based on STRUCTURAL DIFFERENCES
Immunoassays
Polyclonal or monoclonal antibodies toward the glycated n-terminal group of the β chain of Hgb
Affinity chromatography
Separates based on chemical structure using borate to bind glycosylated proteins
Not affected by temperature and other hemoglobins
Methods based on CHARGE DIFFERENCES
Ion-exhange chromatography
Positive-charge resin bed
Highly affected by temperature and hemoglobinopathies
HbF – ↑
HbS and C – ↓
Electrophoresis
Separation is based on differences in charge
HbF values >7% interferes
Isoelectric focusing
Type of electrophoresis using isoelectric point to separate
Pre-hb A1c interferes
HPLC
Form of ion-exchange chromatography
Separates all forms of glycol Hb (a,b,c)
Advertisements
METHODS FOR ANALYSIS
CHEMICAL
REDUCTION
Cupric Ion Reduction
FOLIN-WU – measure of ALL REDUCING SUBSTANCES in the blood
Reagent that binds with Cu+: phosphomolybdic acid
End product: phosphomolybdenum blue
End color: blue
NELSON SOMOGYI – MEASURE OF TRUE GLUCOSE
Reagent that binds with Cu+: arsenomolybdic acid
End product: arsenomolybdenum blue
End color: blue
NEOCUPROINE
Reagent that binds with Cu+: neocuproine
End product: cuprous-neocuproine complex
End color: yellow/yellow orange
Ferric Ion Reduction – Inverse Colorimetry – reduction of yellow ferricyanide to a colorless ferrocyanide by glucose
HAGEDORN JENSEN
CONDENSATION
Orthotoluidine (DUBOWSKI method)
can be also used for urine and CSF without protein precipitation
Absorbance: 630 nm
Reagent: aromatic amine, glacial acetic acid
End color: green
Interfering substances: galactose and mannose
Polarographic Glucose Oxidase
measures oxygen consumption with PO2 electrode (Clark)
used to avoid interference made by strong oxidizing agents in GOD
Molybdate – catalyzes the oxidation of iodide to iodine by H2O2
Catalase – catalyzes oxidation of ethanol by H2O2 forming acetaldehyde and H2O
Hexokinase
Generally accepted as the REFERENCE METHOD
MORE ACCURATE THAN HEXOKINASE
coupling reaction using G6PD is highly specific
Measured by quantitating reduced NADPH formation
NADPH is measured directly at 340 nm or coupled to chromogen and measured in visible range
May be performed using serum or plasma (heparin, EDTA, fluoride, oxalate & citrate)
Excellent for glucose determination in urine, CSF and serous fluids
OTHER IMPORTANT TESTS
KETONES
Produced by the liver through metabolism of fatty acids to provide ready energy source from stored lipids at times of low carbohydrate availability
THREE KETONE BODIES
Acetone (2%)
Acetoacetic acid (20%)
Β-hydroxybutyric acid (78%)
Causes of increased ketone levels
Diabetes Mellitus
Starvation/fasting
High-fat diets
Prolonged vomiting
Glycogen storage diseases
KETONEMIA – accumulation of ketones in the blood
KETONURIA – accumulation of ketones in the urine
MEASUREMENT OF KETONES
For patients with Type 1 Diabetes, it is recommended during acute illness, stress, pregnancy, or elevated blood glucose levels above 300 mg/dL or when patients have signs of ketoacidosis
SPECIMEN: FRESH SERUM or URINE tightly stoppered and analyzed immediately
METHODS FOR ANALYSIS:
GERHARDT’S TEST – historical test
Used FERRIC CHLORIDE reacted with ACETOACETIC ACID to produce a RED color
SODIUM NITROPRUSSIDE – more common method
Uses SODIUM NITROPRUSSIDE which reacts with ACETOACETIC ACID in an ALKALINE pH to form a PURPLE COLOR
If GLYCERIN is also added, ACETONE will be detected
Used in urine reagent strips and Acetest tablets
ENZYMATIC – newer method adapted in some automated intstruments
Uses β-HYDROXYBUTYRATE DEHYDROGENASE to detect either β-HYDROXYBUTYRIC ACID or ACETOACETIC ACID depending on the pH of the solution
pH of 7.0 causes the reaction to proceed to the right (decreasing absorbance)
pH of 8.5 to 9.5 causes the reaction to proceed to the left (increasing absorbance)
MICROALBUMINURIA
Defined as persistent albuminuria in the range of 30 to 299 mg/24 h or an albumin-creatinine ratio of 30 to 300 g/mg
Clinical proteinuria or macroalbuminura is established with an albumin-creatinine ratio of ≥300 mg/24h or ≥300 µg/mg
Powerful predictor for future development of diabetic nephropathy
Annual assessment of kidney function by the determination of urinary albumin is recommended for diabetic patients
METHODS FOR MICROALBUMINURIA SCREENING
RANDOM SPOT TEST – preferred method
24-HOUR COLLECTION
TIMED 4-HOUR OVERNIGHT COLLECTION
A patient is determined to have microalbuminuria when two of three specimens collected within a 3- to 6-month period are abnormal.
Factors that may elevate the urinary excretion of albumin include exercise within 24 hours, infection, fever, congestive heart failure, marked hyperglycemia, and marked hypertension
ISLET AUTOANTIBODY AND INSULIN TESTING
Not currently recommended for routine screening for diabetes diagnosis but in the future it might identify at-risk, prediabetic patients
TESTS FOR CARBOHYDRATE DISORDERS
DIAGNOSTIC TESTS
ACTION
Fasting Blood Sugar
Normal – 70-110 mg/dl
Diabetes – >126 mg/dl
2hr Post Prandial Blood Sugar (PPBS)
Normal – <126 mg/dl
Diabetes – >200 mg/dl
Post-Loading Glucose
Similar to PPBS
*Glucose load is standardized
*Diabetics ≥200 mg/dl
Glucose Tolerance Test (GTT) Standard dose = 75g
*Diagnostics of diabetes mellitus
>150 mg/dl after 2 hours
>200 mg/dl after 2 hours
*Perform if FBS and PPBS are normal
Intravenouse Glucose Tolerance Test (IVGTT)
*Poor absorption (flat curve with OGTT)
*Patient who cannot tolerate large glucose load (vomiting)
O’Sullivan Test
(for gestational diabetes)
*Standard dose 50g
*Probable gestational diabetes
>150 mg/dl at 1 hour
*Follow up with OGTT
TESTS FOR MONITORING
NOTES
Glycosylated hemoglobin
*Assessment of long term control
*Average glucose level over 60 days (1-2 months)
Microalbumin
*Detects small amounts of protein in urine of diabetic patients to assess renal damage
The bacteriological examination of water usually consists of
Estimating the number of bacteria present by TOTAL PLATE COUNT
Detecting the presence or absence of coliforms & estimation of the number of coliforms present by the “MOST PROBABLE NUMBER” (MPN) method
DRINKING WATER STANDARDS
U.S. Public Health Service Drinking Water Standards publication
standard for public water supplies
states that NO MORE THAN 10% OF ALL THE STANDARD 10 ml PORTIONS OF WATER EXAMINED IN A MONTH SHALL SHOW THE PRESENCE OF COLIFORM BACTERIA
Sampling
collected in sterile glass containers with ground glass stoppers
should be packed in ice or stored at 6-10°C
examination of contents should be done within
6 hours – IMPURE WATER
12 hours – PURE WATER
20-50 mg of sodium thiosulfate is added to sample bottle when testing water from swimming pools to NEUTRALIZE RESIDUAL CHLORINE and prevent chlorine from killing bacteria in the interval between collection and testing
Two (2) Procedures carried out routinely:
TOTAL BACTERIAL PLATE COUNT – report as number of bacteria (each colony is counted as one bacterium) per mL of undiluted H2O. When bacterial total plate count exceeds 100 organisms/mL at 37°C, the water is usually CONSIDERED UNSAFE FOR HUMAN CONSUMPTION.
TESTS FOR COLIFORM GROUP OF BACTERIA
Coliform group – all AEROBIC & FACULTATIVE ANAEROBIC GRAM NEGATIVE NON-SPOREFORMING BACILLI which FERMENT LACTOSE WITH GAS FORMTION WITHIN 48 HOURS at 35°C.
PRESUMPTIVE TEST
LACTOSE BROTH or LAURYL TRYPTOSE BROTH
POSITIVE: Formation within 48± 3hours of GAS in ANY AMOUNT IN THE FERMENTATION TUBE
NEGATIVE: Absence of gas formation at the end of 48± 4hours incubation
CONFIRMED TEST
BRILLIANT GREEN LACTOSE BILE BROTH FERMENTATION TUBES
POSITIVE: Formation and presence of gas in any amount within 48± 3hours
ENDO or LEVINE’S EMB AGAR PLATES
Results on Endo or Levine’s EMB
Typical nucleated with or without metallic green sheen
Atypical, opaque, unnucleated after 24hour incubation. PINK.
Negative (others)
POSITIVE: Growth of TYPICAL COLIFORM COLONIES with 24± 2 hours
NEGATIVE: Growth of NEGATIVE COLONIES
COMPLETED TEST
BRILLIANT GREEN LACTOSE BILE BROTH FERMENTATION TUBES showing gas used for confirmed test
POSITIVE: Formation of acid and gas in Lactose broth; demonstration of Gram Negative non sporeforming bacilli in the agar
NEGATIVE: Absence of gas formation or failure to demonstrate Gram Negative non sporeforming bacilli in a gas forming culture
THE detection of the coliform group in significant number is takes as evidence of FECAL CONTAMINATION.



 Bilirubin terminology may be challenging for some learners. A helpful tip may be to remember English grammar:
Bilirubin terminology may be challenging for some learners. A helpful tip may be to remember English grammar: VOWELS for B1 (indirect, unconjugated, insoluble)
VOWELS for B1 (indirect, unconjugated, insoluble) Bishop, M. L. (2022). Clinical Chemistry: Principles, Techniques, and Correlations (9th ed.). Jones & Bartlett Learning.
Bishop, M. L. (2022). Clinical Chemistry: Principles, Techniques, and Correlations (9th ed.). Jones & Bartlett Learning.