

- Memory Cell Edition (MCE) — The Comprehensive Online Review Course
- End Cell Edition (ECE) — The Final Coaching Course



Our online review courses are powered by #ThePhoenixxApp© (TPA)
Create an account here and try TPA for free!




MEMORY CELL EDITION (MCE)
Description: A course that aims to provide a comprehensive review of topics PER BOARD EXAM SUBJECT based on the Updated PRC Table of Specifications.
Highlights and Inclusions:
- REVIEW STYLE OPTIONS:
- Scheduled review
- If you like interacting with the lecturer, review assistants, and your online study buddies, join our scheduled review.
- Live Sessions: 9am to 6pm
- See our schedule below
- Self-paced review
- If you are working, or still an undergraduate, or simply prefer to study by your own, you can do self-paced review.
- Hybrid review (combined scheduled and self-paced)
- If you wish to do both, you can. Just maintain your communication with us so we can help you in any way we can.
- Scheduled review
- VALIDITY OF ENROLLMENT:
- Your enrolled subject/s will be VALID UNTIL COVID-19 PANDEMIC ENDS* OR UNTIL YOU TAKE THE BOARD EXAM, WHICHEVER IS SOONER
- *Once the pandemic ends, 1-year validity will follow
- Example scenario: If you enroll today (March 2022) but you plan to take the board exam on March 2023, you can join all the batches of the review with no additional cost. (This offer is valid only during the COVID-19 pandemic.)
- ENROLLMENT OPTIONS:
- Per subject
- Choose this option if you just want to enroll in selected subject/s only or if you do not have the budget yet for a full course review.
- Full course
- Choose this option if you wish to access all subjects right away.
- Get a FREE END CELL EDITION (ECE) COURSE – THE ONLINE FINAL COACHING when you enroll in all subjects (whether in a full course or per subject basis)
- Per subject
- INCLUSIONS:
- Use of ThePhoenixxApp
- Unlimited replays of video lectures
- Download option for offline viewing of videos
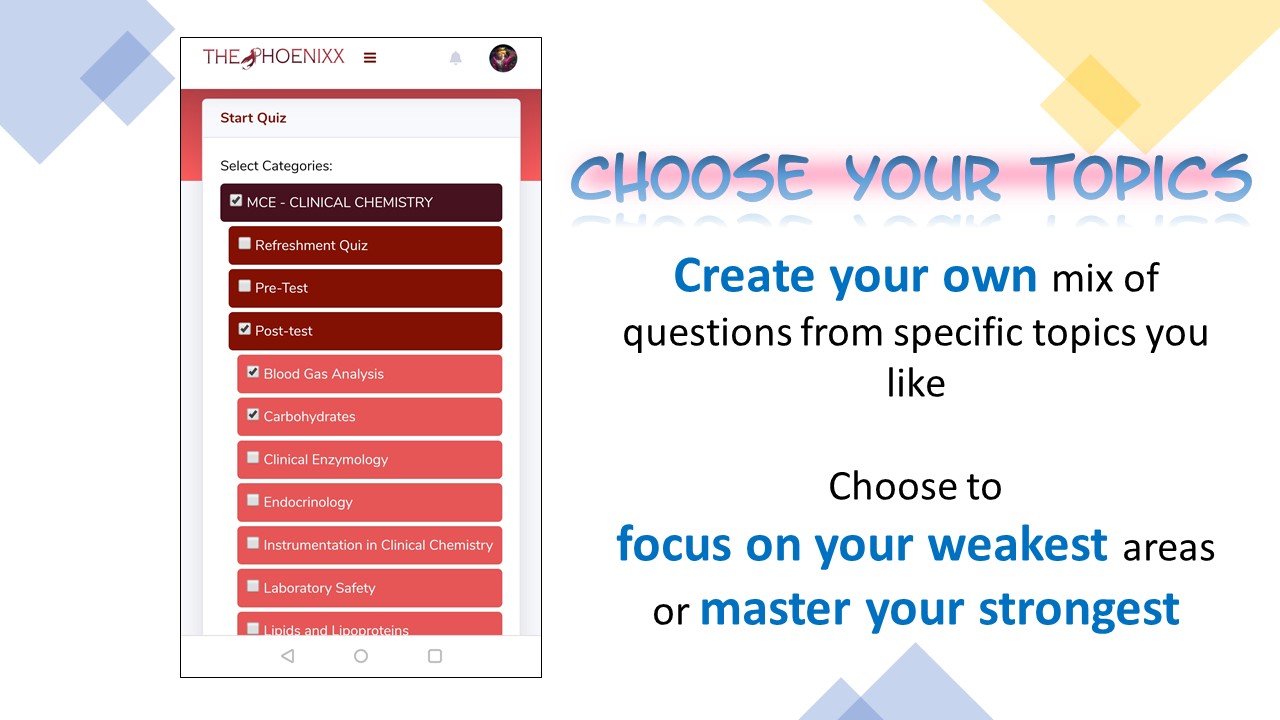
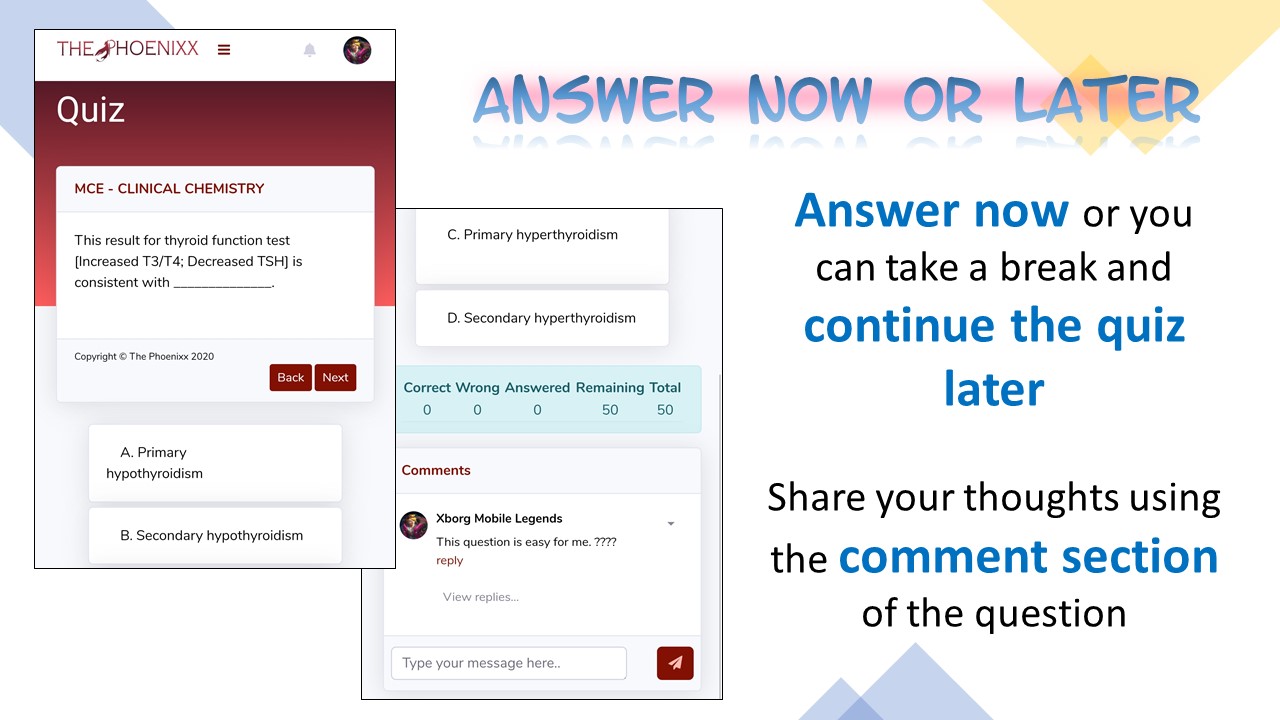
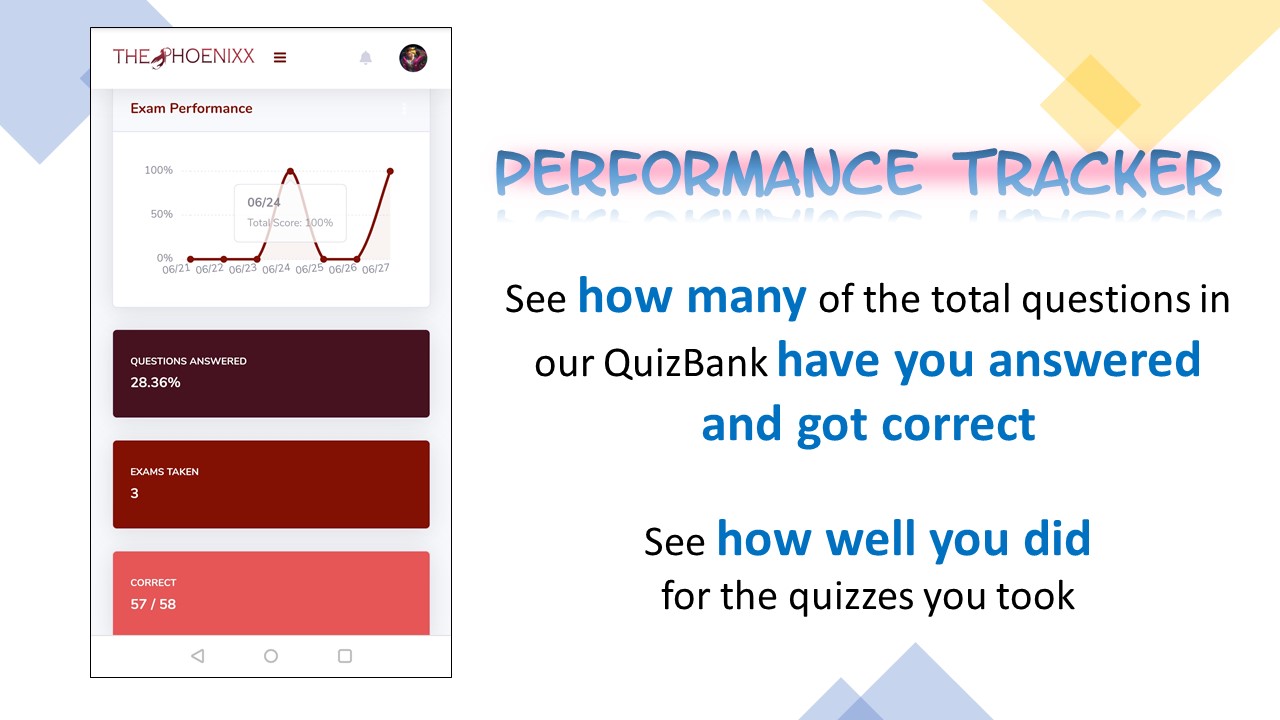
- Practice exams/quizzes with feedback, item analysis, and a progress tracker
- More in-app features to help you be more productive
- Printable and annotatable soft copy of personalized MCE Notes and other review materials
- Every subject (except MolBio*) will have the following academic activities (to be explained in detail during orientation)
- MCE Lectures
- Pre and Post-lecture Exams
- Evaluation Exams with rationalization
- Enhancement Exams with rationalization
- Mastery Sessions
- Drills
- Special lectures for selected subjects
- *MolBio will only include pre/post-test, lecture, and enhancement exams
- GENERAL ACTIVITIES
- Co-MEMORY-ate
- Mock Board Examination
- Brainstorming sessions or virtual group study sessions (Study-With-Me via Discord)
- Small group tutorial (by request)
- EXTRA-CURRICULAR ACTIVITIES
- Worship service/Bible studies
- Mental health hygiene
- Support group
- Chillout sessions
- ZOOMba sessions
- Gaming sessions
- Use of ThePhoenixxApp
Schedule and Review Fees for AUGUST 2024 MCE:
- Dates include INDEPENDENT STUDY TIME (ISTs) or FREE DAY
- NO SUNDAY CLASSES
- You can register now and access the review materials that are already available. Then, you can join the new batch for March 2024 when it begins in November without paying extra.
- UNDERGRADUATES ARE WELCOME TO ENROLL.
| ACTIVITY | TARGET DATES | REVIEW FEE |
| REFRESHMENT WEEK | May 12 to 18, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| MENTAL HEALTH SESSION | May 17, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| GENERAL ORIENTATION | May 18, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| OPENING WORSHIP NIGHT | May 19, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| CC | May 19 to 29, 2024 | P3100 |
| BMVP (Bacte, MycoViroPara) | May 30 to June 10, 2024 | P3100 |
| CM | June 11 to 18, 2024 | P1600 |
| HEMA | June 19 to 28, 2024 | P3100 |
| ISBB | June 29 to July 9, 2024 | P3100 |
| HTMLE | July 10 to 17, 2024 | P1600 |
| MOLECULAR BIOLOGY* | July 18 to 19, 2024 | P1600 |
| Drills | July 20, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| MOCK BOARDS | July 22 and 23, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| Co-MEMORY-Ate | August 3, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| GRAND WORSHIP DAY AND SEND-OFF | August 5, 2024 | FREE FOR ALL MEMORY CELLS AND END CELLS |
| TOTAL FEE | All schedules inclusive of lecture days, ISTs, exams, ratio, and mastery sessions except MolBio (only includes lectures, notes, and enhancement exams) | P17,200* |
*PRICES WILL INCREASE ON AUGUST 1, 2024. Enroll before August 1, 2024, to avail the current prices.
SEE THE SCHEDULE HERE: AUGUST 2024 SCHEDULE
STEPS FOR ENROLLMENT
- REQUIREMENTS:
- Proof of payment (screenshot of transaction or photo of deposit slip/receipt)
- Decent photo to be used for digital ID (preferably graduation pictures)
- Slots for enrollment are unlimited. We can always accommodate you and your friends.
- To get the materials ahead of schedule, please enroll at least 3 days before the subject starts (see schedule here)
- If you were not able to enroll on time, you may still register any time and use ThePhoenixxApp to replay the video lectures
1) When you join, YOU AGREE TO THE FOLLOWING TERMS & CONDITIONS.
a. No recording in any form (audio, video, screenshot) will be allowed. Programs are in place to monitor your in-app activity and once you’ve violated our agreement, we will be compelled to file charges against you.
b. Your personal information will be kept strictly confidential and will not be sold, reused, rented, loaned, or otherwise disclosed.
c. Only fully paid students will be allowed to join. Please BE HONEST and DO NOT invite students to join without paying individually.
2) To proceed with enrollment, please pay first using the following modes of payment. Fees are NON-REFUNDABLE and NON-TRANSFERABLE.
You can pay on a full or per subject basis. (SEE THIS FOR FAQs ABOUT PAYMENT)
To be able to get the materials on time, please enroll at least 3 days before the start of the subject/s.
If the subject/s you are enrolling in is/are already finished, you can still enroll any time as you wish and you will just be replaying the lectures in the app.
| BANK DEPOSIT BANCO DE ORO (BDO) ACCOUNT NAME: Krizza-Almond S. Aguilar ACCOUNT NUMBER: 00 732 001 4669 SECURITY BANK (SB) ACCOUNT NAME: Krizza-Almond S. Aguilar ACCOUNT NUMBER: 00000 17563681 GCASH (See QR code below) If GCASH to GCASH or GCASH to bank, no extra fee If kiosk (i.e., 7-11, palawan) to gcash, please add the required service fee to the amount to be transferred GCash via PALAWAN: add 2% service fee GCash via 7-11: add 3% service fee PLEASE DO NOT SEND PAYMENT VIA PALAWAN PERA PADALA. HUWAG MAGPADALA SA PALAWAN EXPRESS PERA PADALA. |
CLICK THIS FOR THE MCE ENROLLMENT FORM
3) Register using this MCE form. Please make sure you have the proof of payment ready as well as a decent photo which we will be using for your digital ID.
4) Wait for confirmation via text or email along with the instructions. Sir Axel will assist you. Kindly wait for his message.

WHO CONDUCTS THE LECTURES?
Dra. Krizza-Almond S. Aguilar-Salido handles all lectures for the 7 subjects but there will be invited special lecturers for a the exam rationalizations and special sessions.







